
Timings : 6 PM to 8 PM

BOOK APPOINTMENT
9810076517, 011-40392563
9810076517, 011-40392563
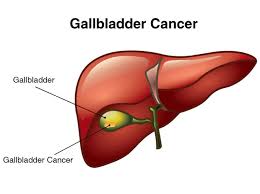 The gallbladder is a small, pear-shaped organ under the liver. The gallbladder concentrates and stores bile, a fluid made in the liver. Bile helps digest the fats in foods as they pass through the small intestine.
The gallbladder is a small, pear-shaped organ under the liver. The gallbladder concentrates and stores bile, a fluid made in the liver. Bile helps digest the fats in foods as they pass through the small intestine.
When food (especially fatty food) is being digested, the gallbladder squeezes and sends bile through a small tube called the cystic duct. The cystic duct joins up with the common hepatic duct (which comes from the liver) to form the common bile duct. The common bile duct joins with the main duct from the pancreas (the pancreatic duct) to empty into the first part of the small intestine (the duodenum) at the ampulla of Vater.
The type of cancer tells you which type of cell it started in. There are several types of gallbladder cancer.
So if the cancer started in gland cells, it is an adenocarcinoma. If it started in the skin like cells lining the gallbladder, it is a squamous cell cancer, and so on.
This is the most common type of gallbladder cancer. More than 85 out of every 100 gallbladder cancers (85%) are adenocarcinomas. The cancer starts in gland cells in the gallbladder lining.
There are three types of adenocarcinomas of the gallbladder. You might hear your doctor talking about.
 Squamous cell cancers develop from the skin like cells that form the lining of the gallbladder, along with the gland cells. They are treated in the same way as adenocarcinomas. Only about 5 out of every 100 gallbladder cancers (5%) are squamous cell cancers.
Squamous cell cancers develop from the skin like cells that form the lining of the gallbladder, along with the gland cells. They are treated in the same way as adenocarcinomas. Only about 5 out of every 100 gallbladder cancers (5%) are squamous cell cancers.
Other rare kind of gall bladder cancers are Adenosquamous cancer, small cell cancer, sarcomas, neuroendocrine tumors and lymphomas.
Gallstones. Gallstones are the most common risk factor for gallbladder cancer. These are rock-like formations of cholesterol and bile salts that can occur in the gallbladder or bile duct. Between 80% and 90% of people with gallbladder cancer have a history of gallstones. However, less than 1% of people with gallstones develop gallbladder cancer. It is unknown why some people develop cancer while most with gallstone disease do not.
Gallbladder polyps. This type of polyp is a growth from the inner lining of gall bladder. Gallbladder polyps bulge inward from the inner gallbladder wall. Some polyps may also be caused by inflammation. Gallbladder removal is recommended for polyps larger than 1 centimeter because these are more likely to be cancerous.
Age. Most people diagnosed with gallbladder cancer are older than 70.
Gender. Women are about twice as likely to develop gallbladder cancer as men.
Ethnicity. Mexican Americans and Native Americans, particularly in the southwestern United States, are more likely to develop gallbladder cancer than the general population. Gall bladder cancers are very common in North India in the cities around river Ganga. Exact reason is unknown.
Smoking. Tobacco use may increase the risk of gallbladder cancer.
Family history. A family history of gallbladder cancer slightly increases a person's risk of developing gallbladder cancer.
Symptoms of Gall Bladder Cancer
Sometimes, gallbladder cancer is found unexpectedly after removal of the gallbladder for another reason, such as gallstones or infection of the gallbladder.
Diagnosis of Gall Bladder Cancer
Gall bladder cancer can be detected in two ways. While some cases are detected incidentally in the gall bladder specimen ( incidental gall bladder cancer) others are detected when they have symptoms and investigated ( primary gall bladder cancer) The following tests may be used to diagnose and stage the gallbladder cancer.
Ultrasound. An ultrasound uses sound waves to create a picture of the internal organs. This can detect mass or abnormal thickening in the wall of gall bladder along with stones. It also can tell to some extent about the local spread of cancer to nearby areas lile Bile duct, intestine and liver.
Computed tomography (CECT) scan. A CT scan takes pictures of the inside of the abdomen using x-rays taken from different angles. A computer combines these images into a detailed, 3-dimensional image that shows any abnormalities or tumors. A CT scan can be used to measure the tumor's size. Sometimes, a special dye called a contrast medium is given before the scan to provide better detail on the image. This dye can be injected into a patient's vein and given as a liquid to swallow.
Magnetic resonance imaging (MRI). An MRI uses magnetic fields, not X-rays, to produce detailed images of the body and can be used to find out whether the cancer has spread outside the gallbladder. MRI can be used to measure the tumor's size. A special dye called a contrast medium is given before the scan to create a clearer picture. A special test MRCP is also done with MRI to detect the site of single or multiple blocks in the bile duct due to local spread of cancer.
Endoscopic retrograde cholangiopancreatography (ERCP). An ERCP allows the gastroenterologist doctor to see inside bile duct on Xrays. The person is lightly sedated, and the doctor inserts an endoscope through the mouth, down the esophagus, and into the stomach and small bowel. A smaller tube or catheter is passed through the endoscope and into the bile ducts. Dye is injected into the ducts, and the doctor takes x-rays that can show whether a tumor is present in the area around the bile ducts. A plastic or metal stent can be placed across an obstructed bile duct during ERCP to help relieve jaundice if it is present. This procedure is used more commonly to find cancer of the bile duct than to find gallbladder cancer, but it may also be used if the gallbladder cancer spreads and blocks the bile ducts.
Percutaneous cholangiography. In this procedure, a thin needle is inserted through the skin and into the gallbladder area. A dye is injected through the needle so that a clear image will show up on x-rays. By looking at the x-rays, the doctor may be able to see whether there is a tumor in the gallbladder. More commonly, a cholangiography provides images of the bile ducts, and it may not show a tumor in the gallbladder. However, the procedure is excellent in detecting the site of a blocked bile duct. This procedure is more often done to relieve jaundice or placing stents either before surgery or giving chemotherapy for palliation.
Laparoscopy. Laparoscopy uses an endoscope to look at the gallbladder and other internal organs. The tube is inserted through a small incision in the abdomen. This procedure is done before surgery to know the spread in the abdomen and also to take biopsies.
Blood tests. The doctor may take samples of the patient's blood to check for abnormal levels of bilirubin and other and Liver enzymes when there is a block in bile duct.
Endoscopic ultrasonography. A special endoscope, which is a long flexible scope, is inserted through the mouth after sedation. It can reach the stomach and some of the intestine. It has an ultrasound probe at the end that can be used to look for tumors and guide biopsy with a small needle.
Positron emission tomography (PET) or PET-CT scan. A PET scan is usually combined with a CT scan (see above), called a PET-CT scan. A small amount of a radioactive sugar substance is injected into the patient's body. This sugar substance is taken up by cells that use the most energy. Because cancer tends to use energy actively, it absorbs more of the radioactive substance. A scanner then detects this substance to produce images of the inside of the body. These tests can sometimes be difficult to read because healthy and active tissues also use energy actively.
Fine needle aspiration cytology (FNAC) and Biopsy are usually not done if surgery is being planned to avoid spill of cancer cells. If required it can be done with the help of endoscopic ultrasound from inside. But FNAC/ Biopsy is routinely done if the tumor is non resectable and require chemotherapy.
 Surgery is the removal of the tumor and some surrounding healthy tissue during an operation. This can be done by a GI Oncosurgeon, or hepatobiliary surgeon.
Surgery is the removal of the tumor and some surrounding healthy tissue during an operation. This can be done by a GI Oncosurgeon, or hepatobiliary surgeon.
Cholecystectomy. Also called a simple cholecystectomy, this procedure involves the removal of the gallbladder. An extended cholecystectomy is the removal of the gallbladder, 1 inch or more of liver tissue located next to the gallbladder, and all of the lymph nodes in the region.
Radical Gallbladder Resection. This procedure involves the removal of the gallbladder, a wedge-shaped section of the liver near the gallbladder, the common bile duct, part or all of the ligaments between the liver and intestines, and the lymph nodes around the pancreas and nearby blood vessels. This surgery may be recommended even if a simple cholecystectomy was already done.
Palliative surgery. Surgery may sometimes help relieve symptoms caused by gallbladder cancer, even if the tumor cannot be removed completely. For example, surgery may relieve a blockage of the bile ducts or intestines, or relieve bleeding.
All these type of surgeries can be performed by making a big cut in the abdomen ( open method ) or my minimally invasive technique ( By making small wholes in abdomen wall). Advantage of minimally in evasive technique has the advantage of faster recovery, less pain and faster discharge from the hospital.
Radiation Therapy
Radiation therapy is the use of high-energy x-rays or other particles to destroy cancer cells. A doctor who specializes in giving radiation therapy to treat cancer is called a radiation oncologist.. A radiation therapy regimen, or schedule, usually consists of a specific number of treatments given over a set period of time.
Radiation therapy may be used before surgery to shrink the size of the tumor or after surgery to destroy any remaining cancer cells. In some cases, radiation therapy is given during surgery to directly target the area of the tumor and protect healthy organs from the effects of traditional radiation therapy. This procedure is called intra-operative radiation therapy, or IORT.
Radiation therapy may also be combined with chemotherapy, a treatment called chemoradiotherapy. Chemoradiotherapy may sometimes be given after surgery and chemotherapy to destroy remaining cancer cells when there is a positive margin that can be seen with a microscope. A positive margin means that there are cancer cells around the area where the tumor was removed.
Radiation therapy is not always used for gallbladder cancer, so your doctor may or may not recommend it.
Chemotherapy
Chemotherapy is the use of drugs to destroy cancer cells, usually by ending the cancer cells' ability to grow and divide. A chemotherapy regimen, or schedule, usually consists of a specific number of cycles given over a set period of time. A patient may receive 1 drug at a time or a combination of different drugs given at the same time.
Chemotherapy should be given after surgery to help prevent a recurrence. ASCO recommends capecitabine (Xeloda) for 6 months after surgery. People with hilar cholangiocarcinoma and extrahepatic cholangiocarcinoma may receive chemoradiotherapy after surgery and capecitabine to destroy remaining cancer cells when there is a positive margin that can be seen with a microscope. A positive margin means that there are cancer cells around the area where the tumor was removed (see Radiation Therapy, above, for more on the ASCO recommendations).
Other drugs commonly used to treat gallbladder cancer include gemcitabine (Gemzar), fluorouracil (5-FU), cisplatin (Platinol), and oxaliplatin (Eloxatin). The side effects of chemotherapy depend on the individual and the dose used, but they can include fatigue, risk of infection, nausea and vomiting, hair loss, loss of appetite, and diarrhea. These side effects usually go away after treatment is finished.
Chemotherapy is usually used as a palliative care treatment for gallbladder cancer. It may be recommended after the tumor has been removed surgically. Chemotherapy used before surgery is called neoadjuvant therapy. And chemotherapy used as an additional therapy after surgery is called adjuvant chemotherapy.