
Timings : 6 PM to 8 PM

BOOK APPOINTMENT
9810076517, 011-40392563
9810076517, 011-40392563
Colorectal Malignancy
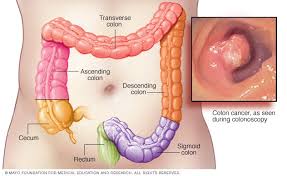
 The large bowel (colon and rectum) is a hollow tubular structure that connects the small bowel to anus. It is of approximately 6 feet in length divided into the caecum, the ascending colon, the transverse colon, the descending colon, the sigmoid colon, and the rectum. The small bowel partially digested contents empty into the caecum through the ileocecal valve and processed in large bowel. The colon removes water, salts and nutrients from the small bowel contents and converted into solid faecal matter (stool).
The large bowel (colon and rectum) is a hollow tubular structure that connects the small bowel to anus. It is of approximately 6 feet in length divided into the caecum, the ascending colon, the transverse colon, the descending colon, the sigmoid colon, and the rectum. The small bowel partially digested contents empty into the caecum through the ileocecal valve and processed in large bowel. The colon removes water, salts and nutrients from the small bowel contents and converted into solid faecal matter (stool).
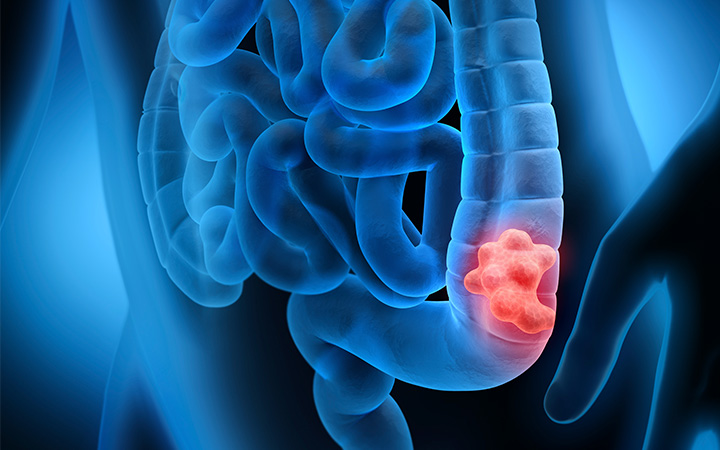
Cancer may begin in the inner lining (mucosa) of any part of colon or rectum and they are collectively called colorectal cancer. Most colorectal cancers start as a polyp but every polyp is not a cancer. The polyps with thick base and fleshy in texture also called adenomas which can become cancer. Colorectal cancer is one of the leading causes of cancer-related deaths worldwide. Early diagnosis of colorectal cancer can often lead to a complete cure. If untreated, bowel cancer can spread locally into the deeper layers of the bowel wall. It can spread from bowel wall to the lymph nodes and further to other organs, such as the liver, lungs and peritoneal surface ( covering gastrointestinal organs and inner surface of abdominal wall ) often called metastasis.
Colorectal cancer arises from gland of the inner lining is called adenocarcinoma comprises 95%. Other types of cancer that arise from other component of large bowel include lymphoma, neuroendocrine tumors, melanoma, and GIST
The risk factors of Colorectal Malignancy
The exact cause of bowel cancer is not known. However, some probable risk factors that increase the chance of developing colorectal cancers are -
Older age : most commonly affects people over the age of 50.
Male gender - more common in male.
Large bowel diseases : people who have long standing inflammatory bowel disease, such as Crohn's disease or ulcerative colitis for more than 10 to 20 years.
Change in lifestyle factors : a lack of physical exercise, obesity, a diet high in fat or animal products (red meat), high alcohol consumption and smoking.
Inherited genetic conditions - Certain genetic conditions running in families that cause a small number (5% to 6%) of large bowel cancers like Familial adenomatous polyposis (FAP) and hereditary non-polyposis colorectal cancer (HNPCC).These condition causes numerous polyps to form in the bowel and if polyps are not removed, they become cancerous.
Family history of cancer - If one or more of the family members (such as a parent, sibling or grandparent) have been diagnosed with bowel cancer, it may run in the family. People are at risk if two relatives on the same side of the family have cancer, or if they were diagnosed before the age of 55.
The symptoms and signs of colorectal cancer depend on the location of tumor in the large bowel and whether it has spread elsewhere in the body (metastasis)
The classic warning signs include :
Change in bowel habits such as worsening constipation or diarrhea
Blood in the stool either bright red or very dark in color
Decrease in stool caliber
A feeling of incomplete evacuation
Loss of appetite
Unexplained weight loss
Weakness and fatigue
Cramping or steady abdominal pain, nausea or vomiting
Anemia
May feel Lump in the abdomen
Diagnosis of Colorectal Cancer
 Medical history evaluation and Physical examination - If signs or symptoms suggest colorectal cancer, complete medical history including risk factors and family history are evaluated in detail.
Medical history evaluation and Physical examination - If signs or symptoms suggest colorectal cancer, complete medical history including risk factors and family history are evaluated in detail.
In physical examination especially abdomen of the patient is examined for abdominal lump and or enlarged organs, A digital rectal exam (DRE) is done in which a lubricated, gloved finger is introduced into the rectum to feel for any abnormal rectal growth.
Not everyone who has the above symptoms has bowel cancer. Other medical conditions, such as hemorrhoids or anal fissure, and some foods or medications, can also cause these changes. If patients has any of the above symptoms for more than two weeks to confirm the diagnosis and to exclude benign diseases certain investigations are done.
Blood test - complete blood count (CBC) is done to rule out anemia. Some people with colorectal cancer become anemic because of prolonged bleeding from the tumor.
Liver function test -in advanced colorectal cancer sometimes liver enzymes are raised due to spread of cancer cells to the liver.
S.CEA is a tumor marker which is needed in the post operative period as a follow up tool
Barium enema -it is widely available and may be used to investigate patients with symptoms suggesting of colorectal carcinoma. Thin barium is passed into large bowel through anus and abdominal x-rays are taken to localize the tumor. With wide spread availability of colonoscope this test is seldome done now a days.
Colonoscopy -in this test a small diameter endoscope is passed through anus in large bowel to examine the inner surface. When viewed through the endoscope, the vast majority of colon and rectal cancers are endoluminal masses that arise from the mucosa and protrude into the lumen. It is the most accurate and versatile diagnostic test for colorectal cancer since it can localize and biopsy lesions throughout the large bowel.
CT colonography -it is also called virtual colonoscopy or CT colography. The air-filled distended colon is examined by CT scan and final picture is processed by software. CT colonography is done in those patients in whom complete colonoscopy can't be performed due to luminal blockage.
Histopathological examination of colonoscopic biopsy -small pieces of abnormal tissues are taken during colonoscopy and are examined under microscope to confirm the diagnosis of colorectal malignancy.
Genetic tests on biopsy tissues -genetic analysis by a trained pathologist is done for changes in the KRAS, NRAS & BRAF gene. Patients with cancers with mutations in either of these genes do not benefit from targeted gene such as cetuximab and panitumumab. IHC for microsatellite instability is also done in some cases.
Serum carcinoembryonic antigen (CEA) -this is the Tumor marker for colorectal malignancy. However, this marker has a low diagnostic ability to detect primary colorectal malignancy due to significant overlap with benign disease and low sensitivity for early-stage disease. Elevated preoperative CEA levels that do not normalize following surgical resection imply the presence of persistent disease and the need for further evaluation. A rising CEA level after surgical resection implies recurrent disease and should prompt follow-up radiologic imaging.
Once the diagnosis of colorectal cancer (CRC) is established, the local and distant extent of disease (staging) is determined by CT Abdomen/Chest scan, MRI Pelvis and PET scan to provide a framework for discussing therapy and prognosis
CT scan -colorectal cancer patients undergo chest, abdomen, and pelvic CT scanning which can demonstrate regional tumor extension, regional lymphatic and distant metastases, and tumor-related complications (eg, obstruction, perforation, fistula formation.
MRI abdomen and pelvis -In current practice, liver MRI is generally reserved for patients who have suspicious but not definitive findings on CT scan, particularly if better definition of hepatic disease burden is needed in order to make decisions about potential hepatic resection. Dedicate MRI Pelvis is mandatory in all rectal cancer patients to have local staging.
Positron emission tomography (PET) scans -PET scan does not appear to add significant information to CT scans for routine preoperative staging of colorectal malignancy. It s role is in localizing sites of disease recurrence in patients who have a rising serum carcinoembryonic antigen (CEA) level and nondiagnostic conventional imaging evaluation following primary treatment.
Endorectalultrasound : This test uses a special transducer that is inserted directly into the rectum to see how far through the rectal wall a cancer may have penetrated and to examine spread of cancer to nearby organs or lymph nodes.
Surgical resection - Removal of segment of colon (colectomy) or rectum (proctectomy) along with adjacent lymph nodes is the main stay treatment. In colon cancers adjuvant ( post operative ) chemotherapy is used in stage II/III. In stage II/III rectal cancers Radiation and chemotherapy (neoadjuvant CRT) is used to down stage the tumor and reduce chances of local recurrence.
Chemotherapy is aimed at trying to destroy any remaining cancer cells. For patients with rectal cancer with this stage, radiation therapy is usually given in combination with chemotherapy, either before or after surgery.
Stage IV (metastatic) colorectal cancerIf cancer has spread to distant organ in the body like liver, lung, ovaries, peritoneum, it is called metastatic cancer. Recommend treatment includes a combination of, radiation therapy, chemotherapy and surgery. The aim of this treatment protocol is to slow the spread of the disease and often temporarily shrink a cancerous tumor. Supportive care is also required to help relieve symptoms and side effects.
Surgery is done for palliation to relieve the blockage of the colon and to control excessive hemorrhage from tumor. Surgery is also required to remove parts of other organs that contain cancer cells e.g. limited spread (metastasis) to liver or lung.
If the cancer has spread only to the liver or lung and if surgery is possible-either before or after chemotherapy-the patient has a chance of complete cure. If cure is not possible then surgery can prolong the life span
 If the cancer reappears after the definitive treatment, it is called recurrent cancer. It can develops in the same place (local recurrence), close to original site (regional recurrence), or in distant organ (distant recurrence). After a battery of investigation and clinical examination treatment is planned accordingly. Treatment option includes chemotherapy, radiation therapy and surgery in a different combination. Most of the times the treatment options for recurrent cancer are the same as those for metastatic cancer.
If the cancer reappears after the definitive treatment, it is called recurrent cancer. It can develops in the same place (local recurrence), close to original site (regional recurrence), or in distant organ (distant recurrence). After a battery of investigation and clinical examination treatment is planned accordingly. Treatment option includes chemotherapy, radiation therapy and surgery in a different combination. Most of the times the treatment options for recurrent cancer are the same as those for metastatic cancer.
If treatment fails
A patient who has advanced cancer where successful treatment is not possible, palliative care called hospice care is advised. The aim of palliative care is to provide a comfortable pain free life.
Chemotherapy
Chemo is typically given as well, before and/or after surgery with or without radiotherapy. The main options for chemo for this stage include 5-FU and leucovorin (alone) or with capecitabine and oxaliplatin regimens are used based on the staging of the tumor and general condition of the patients. If the metastases cannot be surgically removed because they are too large, chemo may be tried first to shrink the tumors to allow for surgery. Most patients with stage IV cancer will get chemo and/or targeted therapies to control the cancer. The most commonly used regimens are FOLFOX (5-FU, leucovorin, and oxaliplatin), FOLFIRI (5-FU, leucovorin, and irinotecan) and CapeOX (capecitabine and oxaliplatin). Sometimes targeted therapies either bevacizumab or cetuximab are also including with regular chemotherapy regimen in cases of advanced and metastatic cancer.
If the only site of cancer spread is the liver, chemotherapy is given directly into the artery (hepatic artery infusion) as hepatic metastasis takes their direct supply from artery. This may shrink the cancers in the liver more effectively than if it is given intravenously or orally.
If the chemo shrinks the tumor and in some case if surgery may become possible then chemotherapy is again used after the surgery.
Radiotherapy
Mostly radiotherapy is given in combination with chemotherapy for rectal cancer either in the form of neoadjuvent or adjuvant therapy. It is advised for local cancer control, to kill any remaining cancer cells. For advanced cancers, radiation therapy may also be used to help prevent or relieve symptoms such as pain. Patients who are not healthy enough for surgery, radiation therapy and/or chemotherapy may be the best options. Radiotherapy can be given through anus into rectum directly over the tumor also called endocavitary radiation therapy.
Surgery
For some early small T1 stage I rectal cancers, transanal endoscopic microsurgery is a better option. Tumors are removed through the anus without an abdominal incision. The resected tumor cut surface and margins are examined and If the tumor turns out to have positive margins under the microscope then formal surgery is advised.
Generally for rectal tumor anterior resection (AR), low anterior resection (LAR), ultralow anterior resection and abdominoperineal resection (APR) may be done, depending on exactly where the cancer is found within the rectum from anal verge. For colonic cancer local segmental colonic resection with the draining lymphnodes are done like right radical hemicolectomy or extended hemicolectomy for right colonic cancer and left radical colectomy for left colonic cancers. Except APR, restoration of bowel continuity is done in each case where as in APR a permanent colostomy is created.
In some cases, neoadjuvant (before surgery) or adjuvant (after surgery) chemoradiation is advised for patients depending on the stage of the tumor.
Surgery can be done by either open or minimal invasive methods depending on the tumor condition and availability of the experts. With minimal invasive technique, a telescope is passed into the abdomen while the patient is under anesthesia. The main advantage of minimal invasive method of surgery are smaller incisions, less post operative morbidity, less pain, short hospital stay and similar oncological advantages.
Other options
For liver metastasis another options may include cryosurgery, radiofrequency ablation, or photocoagulation to destroy the tumor.
If the cancer is widespread and not removable with complete luminal occlusion then diverting colostomy may still be needed in some cases. This can relieve or prevent blockage of the colon and so may prevent obstruction. Sometimes, such surgery can be avoided by inserting a stent into the colon during colonoscopy to keep it open.
Palliative care
The main aim of this approach is to provide supportive care to fulfill the physical, emotional, and social needs of a terminally ill patient.
Palliative treatments vary widely and often include medication, nutritional changes, relaxation techniques, and other therapies. Palliative treatments also include chemotherapy, radiation therapy and surgery to eliminate the cancer.
Screening of colorectal malignancy
50 years onwards, every person should be screened regularly for colorectal cancer and continuing until a person is 75 years old.
The traditional screening routine include-
Physical examination- abdominal examination to feel a lump in the abdomen.
Rectal examination - may reveal a mass in patients with rectal cancer.
Complete blood test (CBC) - done to rule out anaemia which is very common in left sided colonic cancer.
Liver function test (LFT) - done to rule out derangement of liver enzymes which are very common in live metastasis.
Fecal occult blood test (FOBT) - may detect small amounts of blood in the stool. This may suggest colon cancer. FOBT must be done along with colonoscopy or sigmoidoscopy to screen for and diagnose colorectal cancer.
Biopsies or tissue samples of any suspicious-looking areas can be obtained during a colonoscopy or sigmoidoscopy for histopathological analysis.
During screening cancer can be detected before symptoms develop. This is when the cancer is most curable.
Screening guidelines are -
In an average risk patient screening for colorectal cancers begin at the age of 50 years and include the following options:
Flexible sigmoidoscopy every 5 years, or
Colonoscopy every 10 years, or
Double-contrast barium enema every 5 years, or
CT colonography (virtual colonoscopy) every 5 years.
Alternatives screening options include include a fecal or stool tests done on a yearly basis.
However, in high risk patient with a family history of colon cancer, screening intervals should begin earlier and be more frequent.