
Timings : 6 PM to 8 PM

BOOK APPOINTMENT
9810076517, 011-40392563
9810076517, 011-40392563
 The bile ducts are slender tubes which travel from the liver to the duodenum (small intestine). They carry a fluid called bile from the liver and gallbladder into the small intestine, where it helps digest the fats in food. Different parts of the bile duct system have different names. In the liver it begins as many tiny tubes (called ductules) where bile collects from the liver cells. The ductules come together to form tubes called small ducts. These merge into larger ducts and then the left and right hepatic ducts. All of these ducts within the liver are called intrahepatic bile ducts.
The bile ducts are slender tubes which travel from the liver to the duodenum (small intestine). They carry a fluid called bile from the liver and gallbladder into the small intestine, where it helps digest the fats in food. Different parts of the bile duct system have different names. In the liver it begins as many tiny tubes (called ductules) where bile collects from the liver cells. The ductules come together to form tubes called small ducts. These merge into larger ducts and then the left and right hepatic ducts. All of these ducts within the liver are called intrahepatic bile ducts.
The left and right hepatic after exiting the liver, join to form the common hepatic duct in an area called the hilum. Lower down, the gallbladder (a small organ that stores and concentrate the bile) is joined to the common hepatic duct by a small duct called the cystic duct. This combined duct is called the common bile duct. The common bile duct passes through part of the pancreas before it joins with the duct of the pancreas and empties into the first part of the small intestine (the duodenum) at the ampulla of Vater.
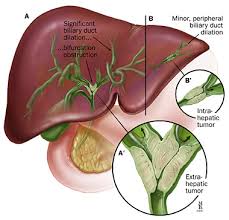
Intrahepatic bile duct cancer: This type of cancer forms in the bile ducts inside the liver. Only a small number of bile duct cancers are intrahepatic.
Extrahepatic bile duct cancer: This type of cancer forms in the bile ducts outside the liver.
 Bile Duct Cancer (Cholangiocarcinoma): Risk Factors and Prevention
The following factors may raise a person's risk of developing bile duct cancer.
Previous disease or irritation of the bile duct. Ulcerative colitis or stones similar to gallstones can cause inflammation of the bile duct. Diseases and conditions that increase the risk of bile duct cancer include:
Bile Duct Cancer (Cholangiocarcinoma): Risk Factors and Prevention
The following factors may raise a person's risk of developing bile duct cancer.
Previous disease or irritation of the bile duct. Ulcerative colitis or stones similar to gallstones can cause inflammation of the bile duct. Diseases and conditions that increase the risk of bile duct cancer include:
Primary Sclerosing Cholangitis (PSC). This is a rare inflammatory condition of the bile ducts. No clearly known cause of this.
Choledochal cyst. This is an abnormality that a person has from birth. It causes ballooning of the part of the bile duct outside the liver.
Caroli syndrome. This is an abnormality of the small bile ducts that a person has in the liver from birth. This syndrome increases the risk of stones and infection in the liver.
Cirrhosis. Cirrhosis is liver disease that can cause scarring or long-lasting irritation. Cirrhosis can have many causes, but hepatitis viruses and alcohol consumption are the most common.
Liver flukes. Liver flukes are parasites that can infect the bile duct, mostly seen in oriental countries.
Age. Older adults are more likely to develop bile duct cancer.
Chemicals. Dioxins, nitrosamines, and polychlorinated biphenyls (PCBs) may cause bile duct cancer. In particular, people who work in rubber plants and automotive industries may be exposed more often to these chemicals.
Jaundice
Jaundice occurs when the bile flow in the intestine is blocked. As a result, bilirubin backs up into the bloodstream and settles in different parts of the body. Jaundice can often be seen as a yellowing of the skin and in the white part (sclera) of the eyes.
Itching
Excess bilirubin in the skin can also cause itching. Most people with bile duct cancer notice itching.
Change in stools
Dark urine
When bilirubin levels in the blood get high, it can also come out in the urine and turn it dark.
Abdominal (belly) pain
Nausea and vomiting
These are not common symptoms of bile duct cancer, but they may occur in people who develop an infection (cholangitis) as a result of bile duct blockage. These symptoms are often seen along with a fever.
Diagnosis of Bile Duct Cancer or Chalingocarninoma
Tests are done to find, or diagnose, cancer. They also done to see whether that has spread to another part of the body from where it started. If this happens, it is called metastasis.
Blood chemistry tests. Blood chemistry tests measure the levels of bilirubin and alkaline phosphatase and check other liver enzymes . High levels of these substances could indicate that the bile duct is not working well.
Tumor marker tests (CEA and CA19-9). Tumor marker tests look for higher-than-normal amounts of certain substances in the blood, urine, or tissues of people with certain types of cancer. Bile duct cancer may cause high levels of carcinoembryonic antigen (CEA) and CA19-9 in the blood. However, a person can have bile duct cancer even if there are normal levels of these tumor markers. Also, there are diseases other than cancer that sometimes cause high levels of these substances.
Other tests may be performed to provide more information about the bile duct cancer. These include:Biopsy. A biopsy is the removal of a small amount of tissue for examination under a microscope by pathologist.
The type of biopsy performed depends on the location of the tumor. The doctor can remove tissue samples during a procedure called a percutaneous transhepatic cholangiography (PTC), which is now rarely used, or another procedure called an endoscopic retrograde cholangiopancreatography (ERCP). Or, a computed tomography scan may help guide a thin needle through the skin into the area to collect a sample of cells.
Other tests can suggest that cancer is present, but only a biopsy can make a definite diagnosis. Occasionally, a biopsy is not possible. In this uncommon situation, people will be treated for bile duct cancer based on other test results and symptoms.
Ultrasound. An ultrasound uses sound waves to create a picture of the internal organs. It may be able to demonstrate the actual tumor. However, more often, the ultrasound will show that the small bile ducts have become larger. This is called a "dilation of ducts." Ultrasound can be used to guide a needle through the skin and into the liver toward a suspected cancer to get a sample tissue for diagnosis.
To view the bile duct, the doctor may alternatively use an endoscopic ultrasound. The doctor inserts a thin, flexible tube, called an endoscope, through the mouth. An ultrasound probe is built into the endoscope. A needle can be passed through the scope to take cells from the mass.
The doctor may also perform an endoscopic retrograde cholangiopancreatography (ERCP). During an ERCP, the doctor inserts a flexible tube down a person's throat, through the stomach, and into the bile duct. Dye is injected into the tube, which helps outline the bile duct on an x-ray. A tiny brush can also be inserted through the tube to collect cells and tissue fragments for a biopsy. This technique can help find and take a sample of the tumor. It provides information that is important in planning treatment.
Less commonly, a surgeon may use a laparoscopic ultrasound. Both of these procedures provide a clearer view of the bile duct. This helps the doctor perform a biopsy.
Computed tomography (CECT) scan. A CT scan takes pictures of the inside of the body using x-rays taken from different angles. A computer combines these pictures into a detailed 3-dimensional image that shows any abnormalities or tumors. A CT scan can be used to measure the tumor's size. A CT scan can also be used to guide a needle to a suspected tumor.
Magnetic resonance imaging (MRI). An MRI uses magnetic fields, not x-rays, to produce detailed images of the body. A specialized MRI used for the bile duct is called MRI cholangiopancreatography (MRCP). A contrast medium may be given intravenously before the MRI to get a clearer picture.
PTC. During this test, a thin needle is inserted into the bile duct in the liver. The doctor injects a contrast medium through the needle that allows the bile ducts to show up on x-rays. By looking at the x-rays, the doctor can tell whether and where there is a blockage of the bile ducts. This method is also utilised for drainage of blocked bile ducts (PTBD).
Laparoscopy. During laparoscopy, a doctor views the bile duct, gallbladder, and liver through a lighted tube, called a laparoscope. The laparoscope is inserted into a surgical opening in the person's abdomen. Some laparoscopes can help the doctor take a tissue sample by using small instruments through the tube.
Surgery
 Surgery is the mainstay treatment of this disease. By surgery the entire tumour along with the the draining Lymph nodes are removed for cure.
Surgery is the mainstay treatment of this disease. By surgery the entire tumour along with the the draining Lymph nodes are removed for cure.
The type of Surgery depends on the location of the tumor. Tumor inside the liver, upper side of bile duct and lower side of bile duct have removal of different organs.
Intrahepatic tumors require removal of either small ( segmentectomy) or large part of liver ( right or left Hepatectomy).
Upper extrahepatic (Hilar cholangiocarcinoma) are treated with removal of right or left hemiliver along with the bile duct and draining lymph nodes while lower cholangiocarcinomas require whipple operation ( removal of Bile duct, gall bladder, Duodenum, Head and neck of pancreas, part of jejunum ( upper small intestine) along with the draining Lymph nodes.
These are major surgeries and are done only when there is potential to cure ( possibility of cure)
Certain procedures may be required before proceeding for major surgeries as above
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy:
It is not yet known whether external radiation therapy helps in the treatment of resectable bile duct cancer. In unresectable, metastatic, or recurrent bile duct cancer, new ways to improve the effect of external radiation therapy on cancer cells are being studied:
Hyperthermia therapy: A treatment in which body tissue is exposed to high temperatures to make cancer cells more sensitive to the effects of radiation therapy and certain anticancer drugs.
Radiosensitizers: Drugs that make cancer cells more sensitive to radiation therapy. Combining radiation therapy with radiosensitizers may kill more cancer cells.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing.
Systemic chemotherapy is used to treat unresectable, metastatic, or recurrent bile duct cancer. It is not yet known whether systemic chemotherapy helps in the treatment of resectable bile duct cancer.
In unresectable, metastatic, or recurrent bile duct cancer, intra-arterial embolization is being studied. It is a procedure in which the blood supply to a tumor is blocked after anticancer drugs are given in blood vessels near the tumor. Sometimes, the anticancer drugs are attached to small beads that are injected into an artery that feeds the tumor. The beads block blood flow to the tumor as they release the drug. This allows a higher amount of drug to reach the tumor for a longer period of time, which may kill more cancer cells.
New types of treatment that may not be standardized yet
Liver transplant
In a liver transplant, the entire liver is removed and replaced with a healthy donated liver. A liver transplant may be done in patients with perihilar bile duct cancer. If the patient has to wait for a donated liver, other treatment is given as needed.
Targeted therapy
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack certain cancer cells. Targeted therapies may cause less harm to normal cells than chemotherapy or radiation therapy do. The following targeted therapies are being studied in patients with bile duct cancer that is locally advanced and cannot be removed by surgery or has spread to other parts of the body:
Immunotherapy
Immunotherapy is a treatment that uses the patient's immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body's natural defenses against cancer. This type of cancer treatment is also called biotherapy or biologic therapy.
Immune checkpoint inhibitor therapy is a type of immunotherapy that may be used to treat bile duct cancer.
Treatment of Unresectable Bile Duct Cancer (Including Metastatic or Recurrent Disease)
Treatment of unresectable (tumors which can not be removed) bile duct cancer (including metastatic or recurrent disease) may include: